For Medical Professionals
Ketamine
Pharmacokinetic Review & Uses in the Anxiety Disorders
A Short History
- 1962 Invented by American scientist Calvin Stevens, Parke Davis Laboratories Derived as a replacement for PCP (veterinarian anesthetic) used since 1926 which was too long lasting and too many dissociative side effects
- 1964 First used on humans
- 1966 Patented in (in Belgium)
- 1970 FDA Approved for clinical use
Used in Vietnam for field anesthesia during combat: A complete anesthesia while providing Cardiovascular and Respiratory Support - Mid-1970s : Argentina Psychotherapists popularized use in Regression Therapy
- 1990’s – Hong Kong : Popular dance culture use combined MDMA (ecstasy) – Regulated as Schedule I, Hong Kong’s Chapter 134, Dangerous Drugs Ordinance.
- 1999: USA Drug Enforcement Administration assigns Ketamine to Schedule III
- 2005: Class C
Federal Regulatory Schedules Defined
| Schedule | Abuse Potential | Legitimate Medical Use | Safety Under Medical Supervision | Dependency Potential | Examples |
| I | High | None | None | Low-High | LSD, MDMA, GHB, Heroin, Peyote, Mescaline |
| II | High | +++ | High | High | Fentanyl, Morphine, Amphetamines, Dilaudid, PCP, Cocaine |
| III | Low | +++ | High | Low | Ketamine, Cough Medicines, GHB, Xyrem, Anabolic Steroids, Cannabinoids |
| IV | Low | +++ | High | Low | Lorazepam, Midazolam, Diazepam, Clonazepam, Phenobarbital, Tramadol, SOMA |
| V | Low | +++ | High | Low | Cough and Appetite Suppressants, Anticonvulsants |
Legal Classifications
| State Drug Class | Legal Penalty for inappropriate possession | ||
| A | Worst Mandatory jail |
Heroine, GBH | |
| B | Moderate Possible Jail |
Cocaine, LSD, Amphetamines, Ecstasy, Oxycotin, Ketamine | |
| C | Moderate Possible Jail |
Ketamine | |
| D | Low Possible Jail |
Marijuana | |
| *A state by state system, not used in California | |||
Pregnancy & Teratogenicity
| Category | Effect on Pregnancy & Teratogenicity |
|
|
| A | None Studies have shown no risk |
||
| B | None-Low Animal Studies = None But no human studies done |
||
| C | Low-Mod Risk <Benefits |
Ketamine | |
| D | Mod High Risk ?<Benefits |
||
| X | High Risk >>Benefits |
||
| N | Unknown or untested therefore no FDA Classification |
Ketamine: Is a 50/50 mixture of both S & R enantiomers
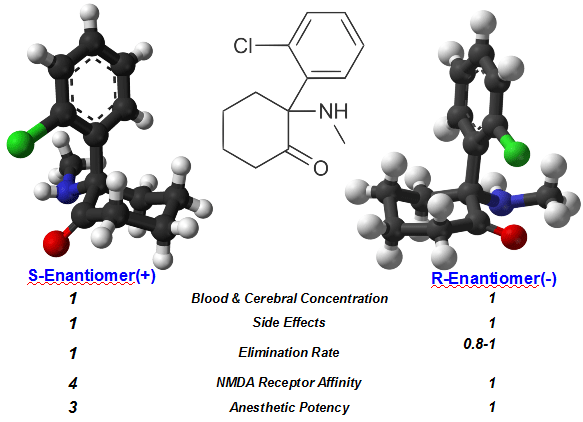
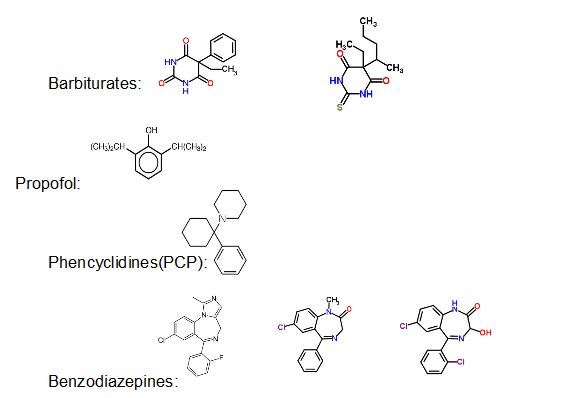
Chemistry:
Despite clinical similarities with other central neuro-modulators the differences are what is most important.
Physiologic Behavior: Receptor Sensitivity
- NMDA Receptors(N-methyl-D-aspartate)-Glutamate or GABA (γ-Aminobutyric acid)
– the main Inhibitory Neurotransmitter in all mammalian CNSs - Mu & Kappa Receptor Spinal Opioid Pain Receptors
not antagonized by Naloxone - C Fibers (more than A-delta) down modulation, Central and Spinal
- Muscarinic – Muscle twitches, motor dis-coordination, etc.
- Anti-cholinergic – Tachycardia, Salivation, etc.
- Serotonin – Brain (assoc. with Depression, Mood, Appetite, Sexual Behaviors), Cardiovascular, GI Tract, Thermoregulation
- Norepinephrine – Sympathomimetic
Many other locations in human body:
CNS locations including hippocampus: learning, cognition, memory centers
Skin, connective tissues, effects uncertain
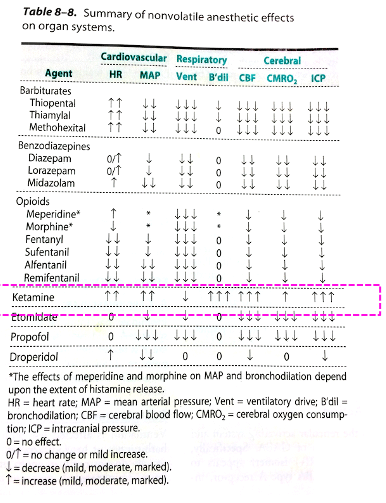
Of significance is to note the cardiovascular, respiratory and cerebral effects of ketamine compared to other anesthetics. These effects make ketamine uniquely useful for specific medical purposes
(Source: Clinical Anesthesiology, Morgan and Mikhail, 5th Edition, 2013, McGraw Hill)
Physiologic Behavior of Ketamine is very useful for…
- Severe Acute Trauma: hypotensive hemorrhage
- Emergency Cesarean Section
- Pediatric Anesthesia
- Surgery of short duration/Intensely painful
- Reactive Airways: Asthma, Emphysema, COPD
- Obstructive Sleep Apnea
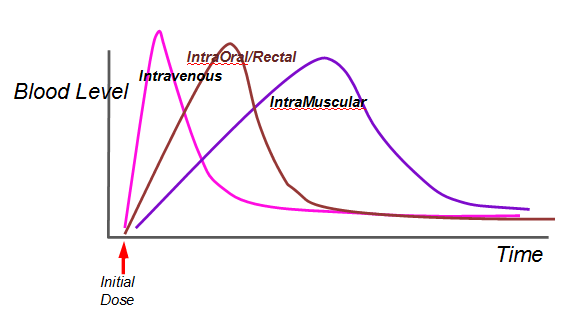
Pharmacokinetics: A Quick Review
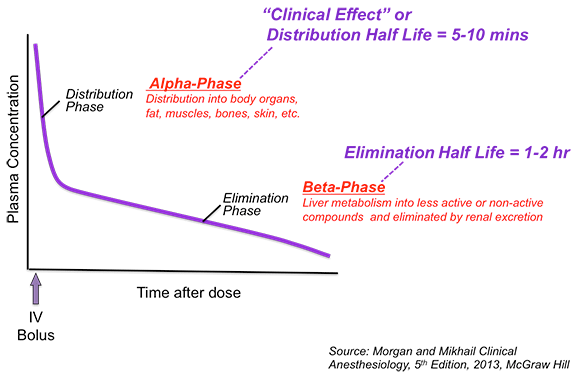
Physiologic Behavior in-situ
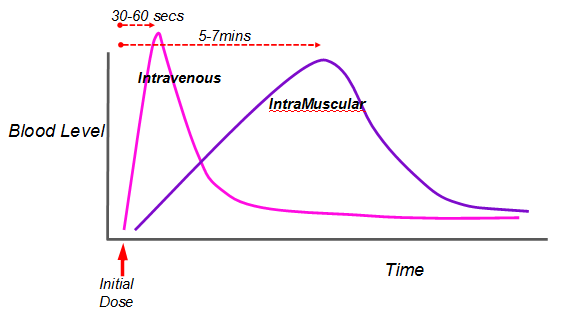
Methods of Dose Administration for an ED50 (general anesthesia):
Intra-Venous: Peak Blood levels 1min.
Intra-Muscular: Peak Blood levels 5min.
Intra-Nasal: 50% bioavailability
Oral: 10%-50% bioavailability
Rectal: 10%-50% bioavailability
Half-Lives: for a single injection
- Alpha: 10-15mins
- Beta: 1-2hrs
- Clinical (surgical anesthesia): 2-5mins
Metabolism:
– Mechanism: 99% is Hepatic p450 conjugation -> NorKetamine (20% potency), Hydroxy-Ketamines (inactive), etc.
– Excretion: Renal
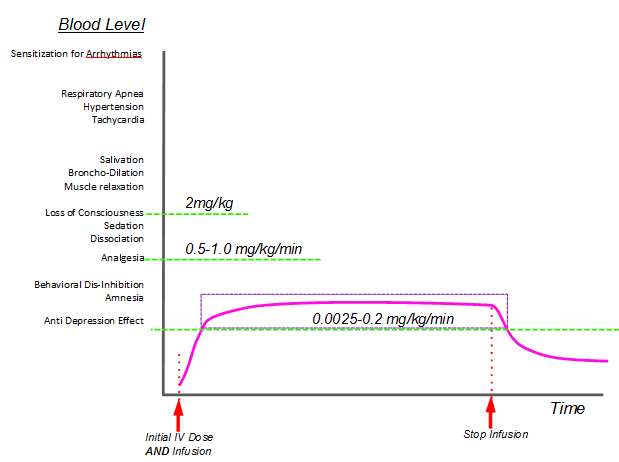
Ketamine’s Clinical Margin of Safety
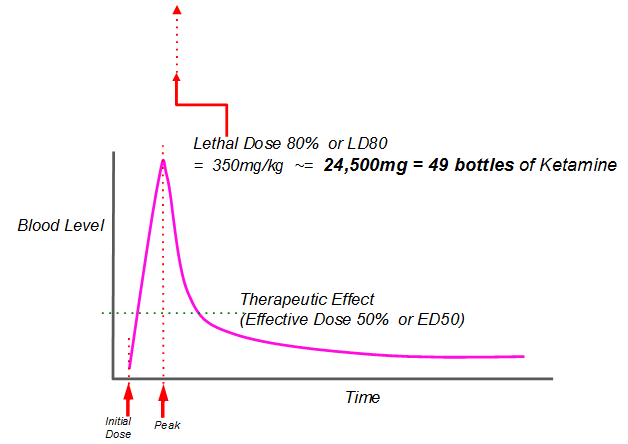
Blood Level & Clinical Effects
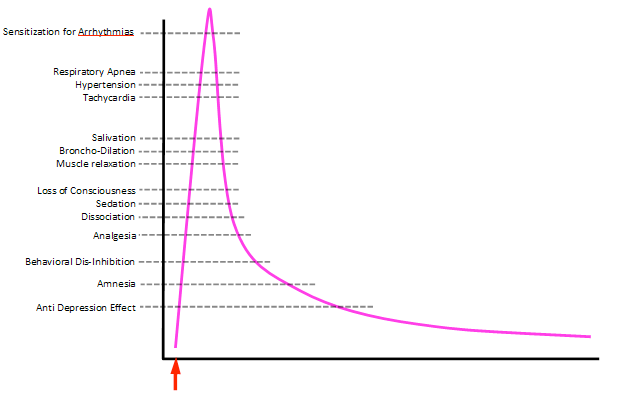
Pharmacokinetics
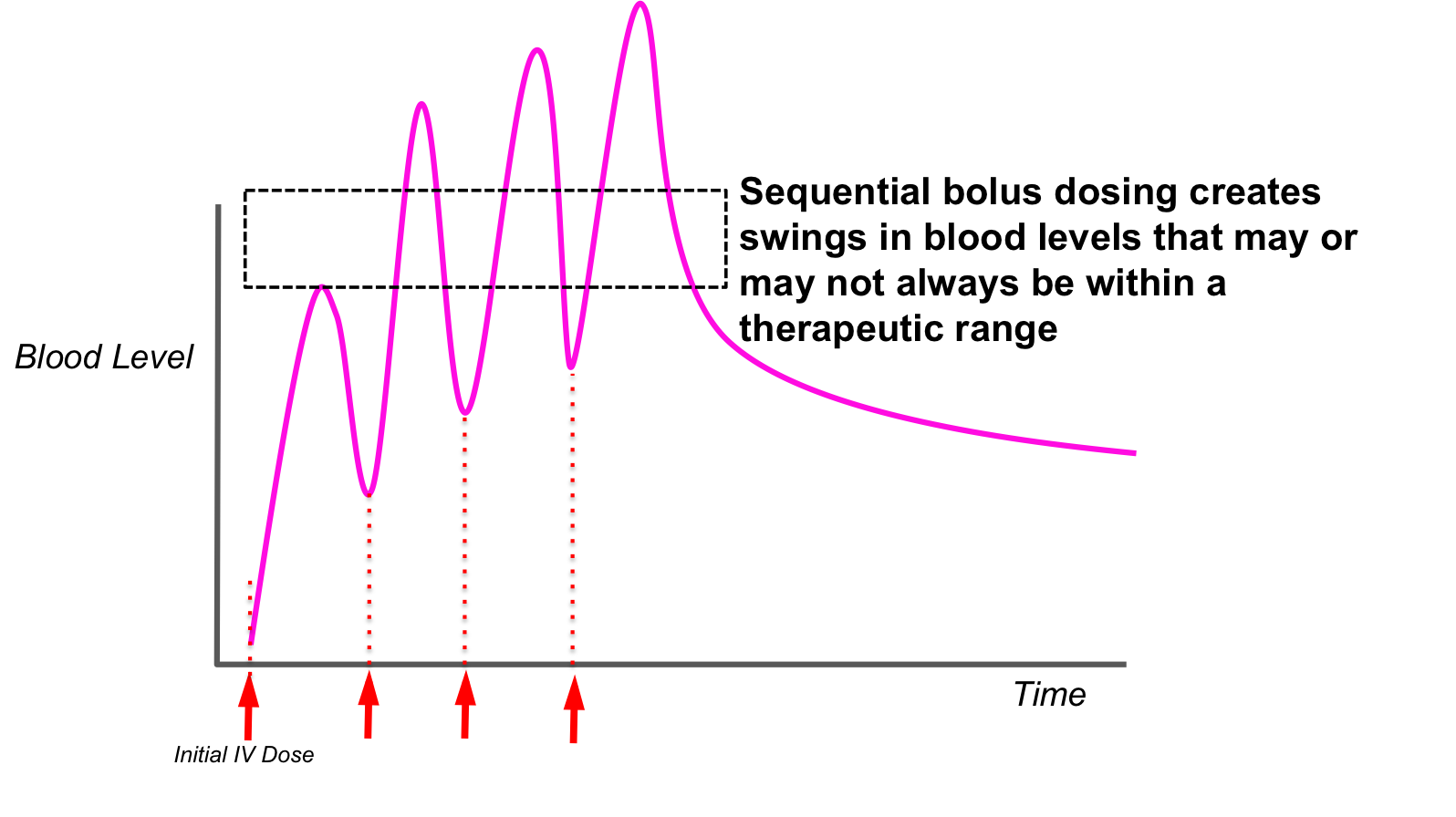
Continual Infusion Dosing achieves a constant therapeutic blood level
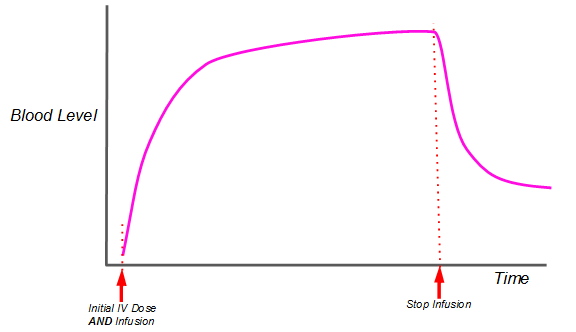
A constant therapeutic blood level over a set amount of time is what is believed to achieve the NMDA Receptor Anti-Depressant effect.
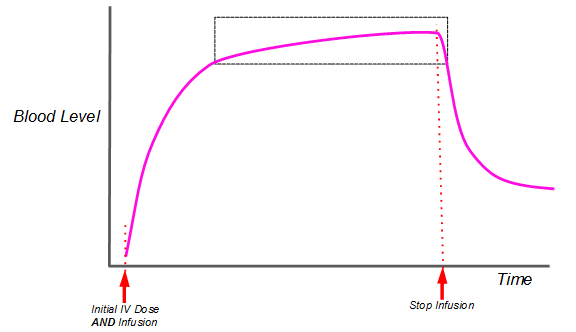
The Anti-Depression Therapeutic Window
A Brief Review of the Anxiety Disorders
- Major Depression
- Dysthymia/Cyclothymia
- Depression-Chronic
- Depression-Cyclic/Acute
- Bipolar Depression
- Suicidal Ideation/Intention (Depressive Emergency)
- Post Traumatic Stress Disorder (PTSD)
- Obsessive Compulsive Disorder (OCD)
- Adolescent Depression
- Post Partum Depression
- General Anxiety Disorders
- Panic Anxiety Disorders
- Social Phobias
Incidence(1): 18.1% of adult population (~40M in USA)
Prevalence(1):
Age < 18: 12.5%
Age 18-29: 30.2%
Age 30-44: 35.1%
Age 45-59: 30.8%
Age 60+ : 15.3%
Societal Cost(2)
Lost Productivity and Disability: ~$217.5 Billion/year in USA
Medical Expenditures: ~$100.1 Billion/year in USA
Sources:
(1)National Institute of Mental Health, www.nimh.nih.gov/health/statistics/cost/index.shtml
(2)Am Journ Psychiatry 2008 Jun; 165(6):663-5
Incidence(1): in Adolescent Population in Guatemala City (1992) 35.1%
Sources:
(1) Berganza CE, Aguilar G.Adolescence. 1992 Winter;27(108):771-82.
Common Co-Morbidities Directly or Indirectly attributed to, or associated with, the Anxiety Disorders.
- Eating Disorders
- Chronic Headaches/Migraines
- Irritable Bowel Syndrome
- Sleep Disorders: Insomnia/Hypersomnia
- Substance Abuse
- Adult ADHD (Attention Deficient/Hyperactivity Disorder)
- Body Dysmorphic Disorder
- Chronic Pain/Fibromyalgia
- Childhood Anxiety Disorders
Sources:
(1)Anxiety and Depression Association of America
The Anti Depressant Mechanism of Ketamine
“We find that ketamine-mediated NMDAR blockade at rest deactivates eukaryotic elongation factor 2 (eEF2) kinase (also called CaMKIII) resulting in reduced eEF2 phosphorylation and desuppression of BDNF translation. Furthermore, we find inhibitors of eEF2 kinase induce fast-acting behavioural antidepressant-like effects. “
Nature. ; 475(7354): 91–95
Anita E. Autry1, Megumi Adachi1, Elena Nosyreva2, Elisa S. Na1, Maarten F. Los1, Peng-fei
Cheng1, Ege T. Kavalali2, and Lisa M. Monteggia
Department of Psychiatry, UT Southwestern Medical Center.
In other words: “…the underlying mechanism is unclear”
- Double Blind Randomized Controlled Cross-Over
- Multi Center
- 24 patients, “Severe Depression”
- All 24 were off all other medications and/or refractory
- Ketamine Dose: 0.5mg/Kg/100 mins
- Intervals: 3x/week x 2 weeks
- Montgomery-Asberg Depression Rating Scale (MADRS)
- Clinician Administered Dissociative States Scale (CADSS)
- Pre-Infusion: 60 mins
- Post-Infusion: 2hrs, 4hrs, 24hrs,
2xweek x4wks,
Every other week x 8weeks,
Total 83 days - Medication free throughout
- Results:
Overall: 70.8% had at least 50% reduction
- Median Time to Relapse: 20 days
- 24% Symptom free @ 83 days
- P<.001
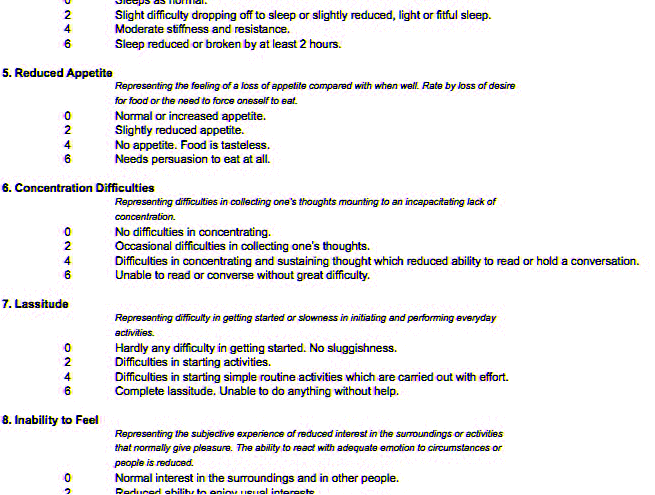
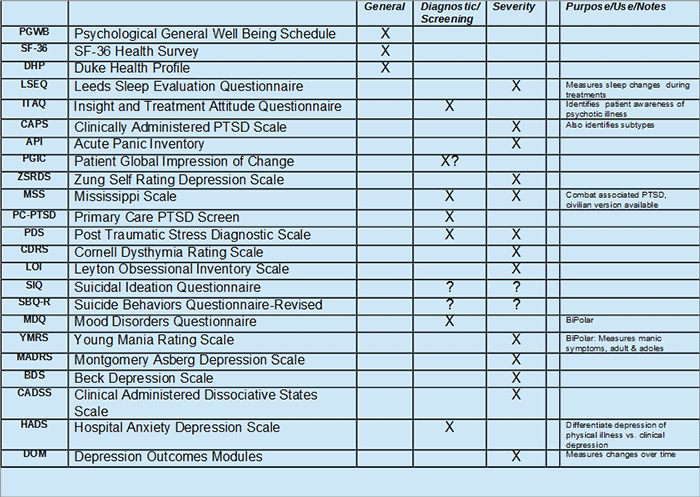
Measurements of Validation & Progress
MADRS: Montgomery Asberg Depression Rating Scale/10 questions
Purpose: Severity of Depression, to measure baseline and long-term effectiveness
Reliability & Repeatability: Correlation Coefficient: 97%, p<.001
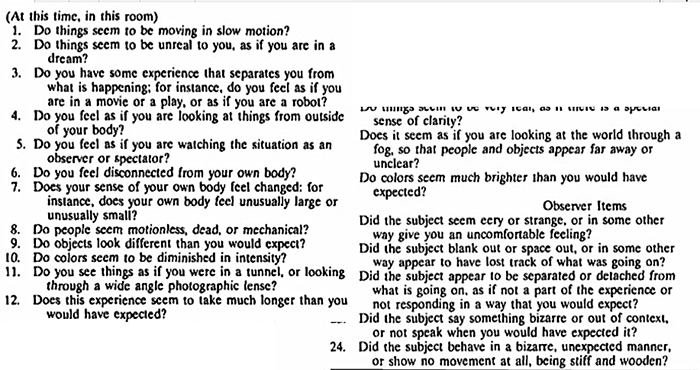
CADSS: Clinician Administered Dissociative State Scale/28 questions
Purpose: Dissociative Symptoms measurement
Pre vs. Post Ketamine Rx -> Ketamine Dosage Adequacy
Reliability/Repeatability: Correlation Coefficient: 94%, p<.0004
CADSS: Clinician Administered Dissociative State Scale
Other Usable Anxiety Testing Rating Scales & Surveys
Depression, the Anxiety Disorders, Ketamine
The IOMI Collaborative
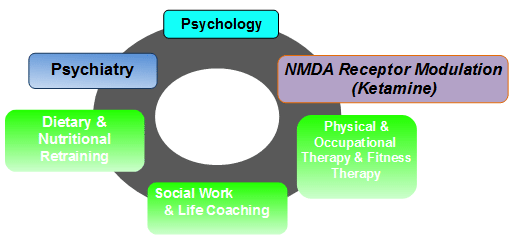
Our Practice-Collaboration
page 34 – need to add screenshot
page35
| Sunday | Monday | Tuesday | Wednesday | Thursday | Friday | Saturday |
|
||||||
| – CADSS – Ketamine Infusion – CADSS |
MADRS | – Ketamine Infusion – CADSS |
– Ketamine Infusion – CADSS |
|||
Ketamine Infusion +-0.5mg/Kg x 50-60 mins
Related and Supportive Studies of note.
Effective for Both Unipolar & Bipolar
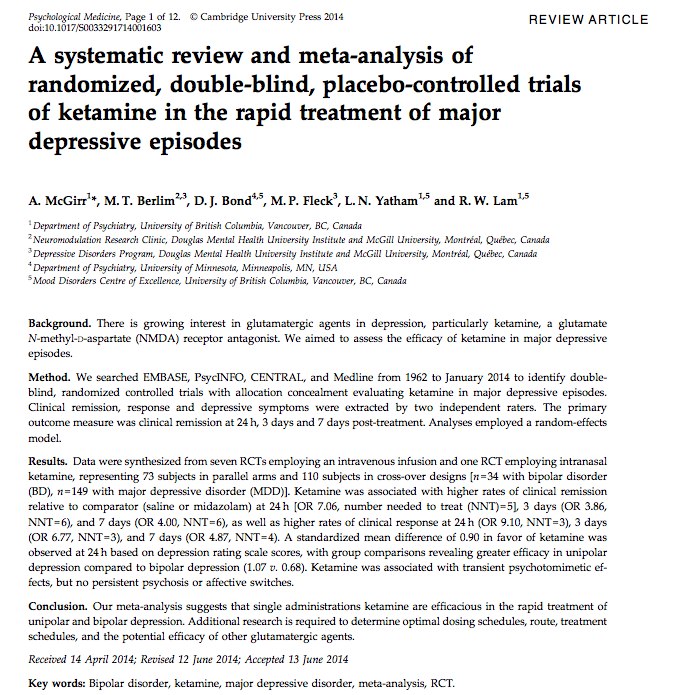
- Meta-Analysis of Double Blind Randomized Controlled Cross-Over (2014)
- 8 studies (7IV, 1 Intra-Nasal)
- Doses: 0.5mg/Kg/40-100 mins
- 24hrs, 3days, 7days
- Results:
– Effective in Unipolar & Bipolar Depression
– The more the better
Serial Infusion is better than a Single Dose
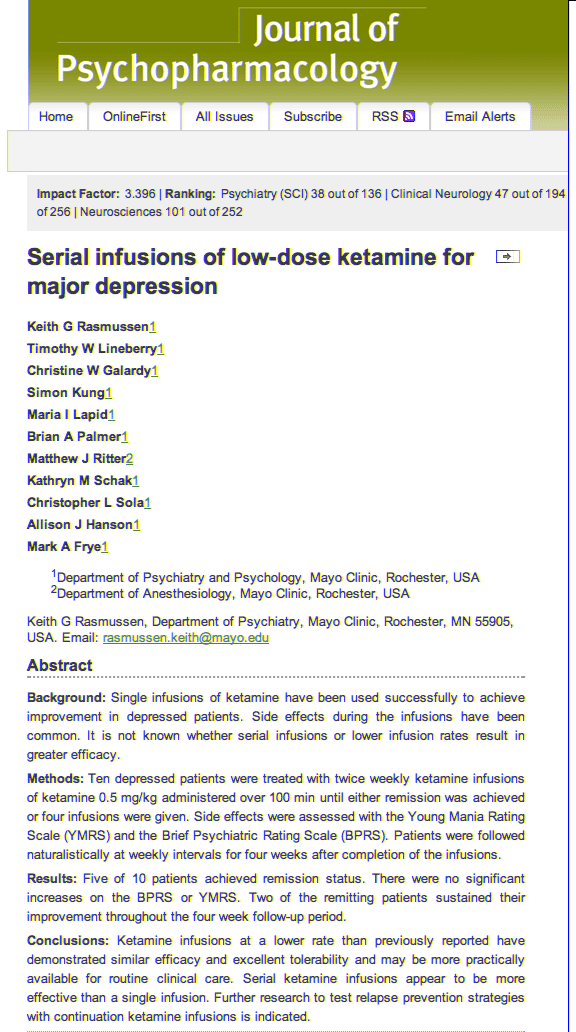
- The Mayo Clinic
- Double Blind Randomized
- 10 patients
- Doses: 0.5mg/kg over 100mins
- Interval: 2/wk up to 4 infus
- Results:
– 50% remission total
– 20% remission x 4 weeks
Post Traumatic Stress Disorder
(PTSD)
- Double Blind Randomized Crossover
Mount Sinai University, Univ. Groningen, The Netherlands - Ketamine vs. Midazolam vs. Placebo
- Intervals: 2/wk up to 4 infus
- Doses: 0.5mg/kg over 100mins
- CADSS, MADRS
- Results:
Greater reduction in symptoms with Ketamine than with Midazolam or Placebo
Ketamine & Suicidal Ideation
- 27 patients 18-65yo
- Dose: 0.5mg/kg/40mins single dose
- SSI & HDRS Scales
– Pre-Infus: 60mins
– Post-Infus: 40mins, 80mins, 120mins, 230mins, 1day, 2days - Decrease Sx:
– 70% @ 40mins
– 45% @ 230Mins - P<0.001
Ketamine vs. Electro-Convulsive Therapy
(ECT)
- Double Blind Randomized Controlled
- 18 patients
- Dose: 0.5mg/Kg/45mins
- Beck Depression Scale & Hamilton Depress RS
- Intervals: 24hrs, 3days, 7days
- Results: Better, sooner, longer than ECT
Ketamine & Obsessive Compulsive Disorder
(OCD)
- Double Blind Randomized Controlled
- Yale University School of Medicine
- 10 patients
- Dose: 0.5mg/Kg/40mins single dose
- Yale-Brown Obess. Convuls. Scale (Y-BOCS)
@ 1,2,3 hrs. & 1, 2, 3, 5, 7, 10, 14, 21, 28 days - Results:
– 70% reduction Sx @ 60mins,
– 35% reduction Sx @ day 3, no significant change thereafter - Conclusion: Effective but with a plateau effect in a single dose modality
Ketamine & Dissociative Side Effects
Journal of Affective Disorders, Apr;159:56-61, 2014
- Randomized Controlled
- 180 patients; Major Depress & Bipolar
- Dose: 0.5mg/Kg/40mins single dose
- CADSS (Clinician Adminis. Dissoc States Scale)
- BPRS (Brief Psychiatric Ratings Scale)
- YMRS(Young Mania Rating Scale)
- HDRS (Hamilton Depress. Rating Scale)
- Results:
Dissociative side effects predict better Anti-Depression response
Exercise & Depression
- Randomized Dual Dose Controlled
- 122 patients, 18-70yo
- Dose:
– Low: 4KKW (3mph walking/75mins / week)
– High: 16KKW (4mph walking /210mins /week) - Interval: 12 weeks
- Scale used: HDRS
- Results: % Remission=
– 4KKW: 5.6% Women, 0.1% Men
– 16KKW: 39% Women, 85% Men
Summary:
Ketamine’s Use in the Anxiety Disorders
- Ketamine is unique among sedative-hypnotics: wide range of receptor targets
- Ketamine has a significant clinical safety profile
- Useful in a variety of Anxiety Disorders, not just Depression
- Infusion Dosing -> better results
- Sequential Treatments -> better results
- Multi-Modality treatment programs appear to improve effectiveness and length of remission